

Since the outbreak was announced on 15 May, significant progress has been made in testing capacities, Tarik Jašarević, spokesperson for the World Health Organization (WHO) informed reporters in Geneva.
Testing for the Bundibugyo virus causing the outbreak is available in six locations in the country: Bunia and Mongbwalu in Ituri Province, Bukavu and Lwiro in South Kivu, Goma in North Kivu, and the capital Kinshasa.
Four additional laboratories have been set up in Uganda where cases had been imported from DRC, with 19 confirmed cases and one probable case identified so far.
Improvements are still needed.
Interrupting the Spread
“We have blind spots with a low number of alerts,” Mr. Jašarević said. “There might be undetected transmission chains. People may still be at risk of infecting others, and we need to identify them”.
Bruno Michon, Operations Manager for the Ebola outbreak at UN partner the International Federation of the Red Cross and Red Crescent Societies (IFRC), emphasized that halting the spread requires investment not only in medical response but also in building trust, which is challenging and time-consuming.
“But in this outbreak, it is crucial. It is lifesaving,” he stated.
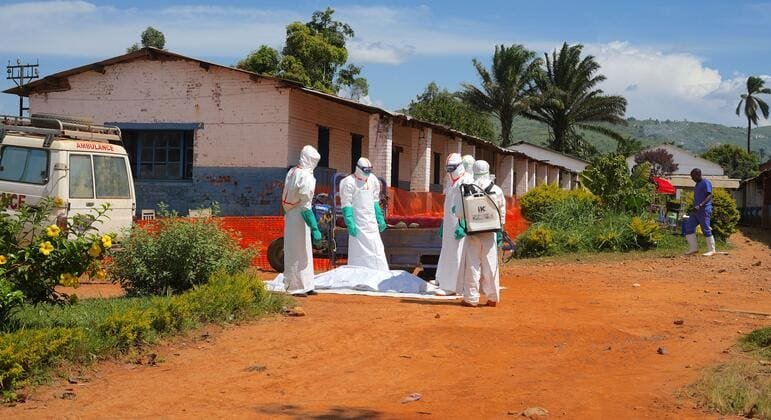
From Bunia, the crisis epicenter, he reported that “some people still doubt the disease’s existence” and think the outbreak could have been “fabricated” to attract foreign aid. Others “view safe and dignified burials as an attack on culture and tradition, rather than a protective measure for families and communities”.
Scepticism, doubt, and fear have slowed the response in conflict-afflicted eastern DRC, with local communities distrusting external authorities, significantly raising disease transmission risks.
Initially, two treatment centers were set ablaze in the region amid heavy fighting, displacing over 100,000 people.
At the time, WHO informed UN News that these attacks were linked to misinformation campaigns on social media.
“When people are afraid, they may not report symptoms,” Mr. Michon explained. “They may avoid treatment centers” fearing contamination and choose to stay home when feverish, “ashamed to tell the family they are sick,” due to the stigma associated with the disease.
“Families try to bury loved ones traditionally without recognizing the risk level,” he added.
Building Trust
The IFRC official stated that trust is built through measures to ease community concerns.
“Based on community feedback, we began using body bags with a window for families to see the deceased’s face” to start the grieving process, he said.
“When communities feared chlorine was poison, we didn’t argue. We demonstrated how disinfectants are made.”
“Without trust, early case detection is impossible,” Mr. Michon continued. “Safe and dignified burials are unfeasible. Family protection isn’t assured, nor can transmission be stopped.”
“Trust isn’t secondary in the Ebola response. It’s central,” he concluded.
Violence Impeding Efforts
As of 14 June, Congolese health authorities reported 808 Ebola cases in Ituri, North Kivu, and South Kivu provinces, the UN humanitarian affairs office OCHA disclosed on Monday.
OCHA cautioned that escalating violence in eastern DRC continues to heavily impact civilians, restrict aid operations, and complicate outbreak containment efforts.
“Continued clashes and resulting displacement raise the risk of Ebola transmission, especially as people move between affected provinces,” the agency noted.
Despite challenges, OCHA and humanitarian partners continue supporting Congolese authorities in containing the outbreak through patient care, enhanced surveillance, preventive measures, risk communication, and providing safe and dignified burials.
Source link






Leave a Reply